„Kolskeggr turned sharp round, and strode towards him, and smote him with his seax on the thigh, and cut off his leg, and said, ‚Did it touch thee or not?’
‚Now,’ says Kolr, ‚I pay for being bare of my shield.’ So he stood a while on his other leg and looked at the stump.
‚Thou needest not to look at it,’ said Kolskeggr, ‚’tis even as thou seest, the leg is off.’
Then Kolr fell down dead.“
(Njáls saga 63)
Thanks to living in one of the safest countries on the planet, a long period of peace and functional medicine, we have forgotten the horrors of war and the scourges of humanity, which makes it difficult for us to assess the quality of life in the past. At the same time, we are unable to fully appreciate the certainties we live in and the hardships our ancestors had to go through. In the following article, we will focus on the neglected issue of amputated limbs due to diseases and war injuries, as well as prostheses of these body parts in the Early Middle Ages. We hope that readers from the ranks of reenactors and those interested in history will find an under-reflected superstructure in the article.
Diseases and injuries of the lower limbs, amputation
Old Norse literature preserves more than fifty bynames that are related to feet (Jónson 1908: 219-223). Many of them relate to leg diseases, legs strangely shaped or legs disabled in a conflict that resulted in a lifetime limping, reflecting the difference or handicap (Sexton 2010). Common diseases affecting legs certainly included ischemia, atherosclerosis, diabetic leg and infections. We can hardly imagine such diseases such as leprosy or polio, which were widespread in the Middle Ages (Hernigou 2014a; 2014b). Medieval injuries had to include fractures and amputation injuries. The most common form of amputation injuries in clinics in non-industrialized countries is the loss of limb or its part, caused by accidents in working with machines, animals, means of transport and falls from a height (Binder 2016: 30). As it seems, the lower limbs below the knee belonged among of the most amputated parts of the human body even in the Middle Ages, together with the hand fingers.

Reconstruction of lower limb fracture fixation around 1350.
Source: van der Mark 2016.
Any injuries were very susceptible to infections that represented a serious medical challenge in the Predantibiotic era (Erdem et al. 2011; Runcie 2015) and which apparently sometimes resulted in amputation; wounds sustained on the British side in WW1 had an infection rate of over 90%. Doctors of the Early Middle Ages were capable of simple surgical operations (cutting, cauterizing and washing wounds, straightening bones) and were able to provide basic care (bandaging, administering herbal infusions, applying stones and herbs, engraving runes and incantations), but they did not have the opportunity to work in a sterile environment, had limited or no knowledge of bacterial infection prevention and their diagnosis was at a pitifully low level by the standards of today’s medicine (Vlasatý 2017). Because of this, the post-operative mortality rate after major surgical procedures was approximately 60-80% (Smith et al. 2012: 36). Because of the high mortality, amputations did not become very widespread before the introduction of modern anesthetics and antiseptics (Van Cant 2018: 199). Amputations were also apparently avoided for the reason that “incomplete people” could be considered incompetent to rule or be marked in the afterlife (Sellegren 1982: 13), or men did not allow amputation due to their pride or doctors refused amputation, saying that they would not bear responsibility for the patient’s mutilation (Friedmann 1972: 117).
Simon Mays (1996) collected a total of 27 archaeological amputations, 5 of which date from the pre-modern period. In three cases, there are amputations of the right lower limbs that are more represented in the finds that Mays did not include (Van Cant 2018: 196). Mays cites three main reasons for amputations in the Middle Ages (Mays 1996: 107):
- surgery associated with illness or combat injury
- surgery associated with a combat injury
- execution of lawful punishment
In contrast, Friedmann (1972: 120) distinguishes a somewhat different spectrum of historical amputations:
- surgery associated with a serious illness
- surgery associated with frostbite
- surgery associated with a combat injury
- severing a limb in an armed conflict
- execution of lawful punishment
Amputations performed due to chronic disease can be expected to a large extent. They are mentioned in written references from the Crusades period (Mitchell 2004) and can also be assumed in the case of some monks whose buried bodies were found near the monastery in St. Petersinsel, Switzerland (Van Cant 2018: 196). Amputations of affected limbs are mentioned in at least two sources from the 11th and 12th centuries. In one case it is a guillotine amputation, in the other it is a flap amputation, which is the more common method today (Janoušek 2015: 18-21). The first of the sources was left to us by the best Arab physician Al-Zahráví, also called Albucasis (Friedmann 1972: 126-127):
“When gangrene of the lower arms or legs does not yield to medication, one should amputate to prevent it extending above the elbow or knee before it becomes fatal. The limb should be slightly bound above and below the line of severance, while an assistant pulls upwards on the upper bandage to retract the skin and flesh. One should make a circular incision down to the bone, insert linen pads on both sides to prevent ulceration, then cut or saw through the bone. If hemorrhage occurs during the operation, cauterize promptly or apply some hemostatic powder before proceeding, apply a suitable dressing and tend until cured.“
The second source is the Lombard translator of Arabic and ancient texts, Gerard of Cremona (Bennion 1980: 51):
“When the malady gets the better of our medicines the limb must be amputated (…) but one remedy, expediency and not safety, is the paramount consideration. We are therefore to make an incision with a knife between the sound and morbid parts down to the bone, with this qualification, that we are never to cut the opposite a joint and always to include some of the sound part rather than leave any of that which is diseased. When we come to the bone the sound flesh must be retracted so as in some measure to denude it; then it must be divided with the saw close up to the sound flesh. The end of the bone is then to be smoothed where the saw has left any asperity and the integuments brought over it, which in this operation, ought to be left loose enough to cover the entire stump as far as possible.“
We have to take these mentions as the peak of surgery at that time, however, we can get basic information from them about how the procedure was carried out. We can see that amputation was a quick affair, taking just a few minutes, and was a team effort involving a surgeon and one or more assistants holding the patient, handing equipment and similar. We often think of operations as being performed without anesthesia, but at least the Persians and Arabs were already using oral or inhaled anesthesia in the Early Middle Ages (Meri 2005: 784). In Viking Age Scandinavia, we know minimum three substances that could be used for these purposes – alcohol, hemp and hyoscyamus (Price 2002: 205-206). It appears that the wounds were often cauterized to stop profuse bleeding, resulting in severe burns that were difficult to heal.
We can agree with Williams (1920: 358) when she says that the early medieval surgeon seems to have most often possessed a saw, a knife, tweezers, a needle and thread. We can assume that the surgeon probably owned several knives, and also had shears or scissors, tweezers, rasps, clamps for closing wounds, and a quantity of clean textiles (Frölich 2011). Desirable attributes of a healer were the “healing hand” (lækshendr, manus medica; according to Magnús saga góða 28, healers were recognized by their soft palms) and “healing tongue” (lyftunga; i.e., healing words, incantations, rune carving, and the ability to communicate with the patient).

A selection of early medieval saws from various European locations.

A selection of early medieval tweezers from various European locations.
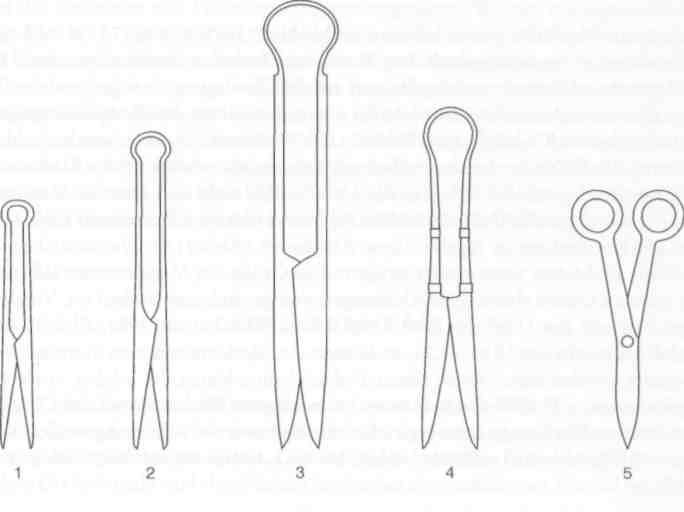
A selection of early medieval shears and scissors. Source: Westphalen 2002: Abb. 32.

A selection of early medieval knives. Source: Westphalen 2002: Abb. 62.
It must be mentioned that even in modern hospitals, the rate of infection of the stump of amputated limbs is around 13-40% (de Godoy et al. 2010). However, successful recovery does not depend only on wound healing – a significant part of patients with successful amputations suffer from psychological problems (Sahu et al. 2016), which need to be addressed to the same extent as physical difficulties. Intensive physiotherapy rehabilitation, which returns the patient to an independent life, is also important (eg Rau et al. 2007); especially in an older age, amputation of the lower limbs is problematic because they are unable to replace the loss with their physical funds, and early death often occurs (Klaphake et al. 2017). About 90% of people with a lower limb amputated below the knee learn to walk with a prosthesis (Pavlačková 2012: 13). It can be said that if the injured person was treated well, quickly and sterile enough, and was in good physical condition, he had a chance to recover and continue with an independent life. In general, it seems that people with prostheses of one lower limb are more successful in getting married, having children and getting a job than people with prostheses of both lower limbs (Claspe – Ramasamy 2013: 71-72). Among other things, the fact that the height of the legs compared to the total height is important for an attractive and healthy appearance may be to blame (Bogin – Varela-Silva 2010).
Head and lower limb injuries appear to be the most common war traumas of the Middle Ages (Matzke 2011: 62-73; Thordeman 1939: 160-178). In Family sagas, warriors commonly lose arms, hands, fingers or legs (Sexton 2010: 152). If we focus on early medieval lower limb injuries, we can mention the leg injury of a man buried in the Gokstad mound in Norway (Holck 2009: 44-46), the shin injury of an early medieval skeleton from Maastricht (Woosnam-Savage – DeVries 2015: 35) or a healed wound on the shin of a member of the massacred garrison of Budeč (Štefan et al. 2016: 766, Table 2). Targeting the lower extremities, especially the shins, makes sense for a number of reasons. The legs make up roughly half the height of an adult person (Bogin – Varela-Silva 2010: 1052-1053), and experiments have shown that even if the wearer has a shield, effective defense of the lower limbs can be difficult for the defender (Matzke 2011: 67 and his own many years of own experience). At least in the Early Middle Ages, there is little evidence of the use of protective equipment for the lower limbs in combat. If the goal was not the definitive elimination of the opponent, hits to the lower limbs could be used intentionally. The head area is three times more susceptible to fatal injuries than the rest of the body (Gennarelli et al. 1989). The tibia is one of the strongest bones in the human body and is rarely broken (Thordeman 1939: 171). Although lacerations of extremities are accompanied by painful agony, death occurs over a long period of time and rescue is therefore possible (Rhyne et al. 1995).

An extreme example of medieval surgery: a humerus found at a monastery in Varnhem, Sweden (SHM 18393:1090) showing a healed fracture caused by an axe. The surgeon attempted osteosynthesis with a copper plate.
Lower limb prostheses
If we want to look at examples of early medieval prostheses, we can use three different sources – archaeology, iconography and written sources.
The history of lower limb prostheses is quite long. Archeology knows of two functional Egyptian wooden thumb prostheses that were made around 1065-600 BC (Finch 2018), as well as a wooden shin covered with a bronze plate from an Italian grave in Santa Maria di Capua Vetere (ca. 300 BC) or a wooden shin tied to the thigh, ending in a horse’s hoof with a horn spike from Shengjindian, China from the same period (Binder 2016: 30). We actually know three finds from the Early Middle Ages, and it is interesting that there are virtually no finds from the Later Middle Ages. The first is a grave from Bonaduz, Switzerland (5th-7th century), which contained a man with his foot amputated at the ankle, replaced by a leather sack filled with a hay-like material with a wooden sole studded with iron nails (Baumgartner 1982). The second find is a wooden left shin prosthesis from Hemmaberg, Austria (6th century), which had a metal socket held by two nails (Binder 2016). The third find is a wood-bronze left shin prosthesis from Griesheim, Germany (7th-8th century), in which the bronze formed a bed for the stump, which was lined with leather, while a wooden fork extended upwards to the level of the thigh, where the straps were attached (Czarnetzki et al. 1983: 91-92). A lower limb prosthesis can also be assumed in case of a man from the Swiss locality of Aesch (7th century), who lived roughly 1-2 years after amputation (Cueni 2009: 115-118). It is evident from this list that each prosthesis was unique, and therefore there was variability in shapes and materials. We can note that in addition to functionality, comfort and aesthetic quality of prostheses are also important.
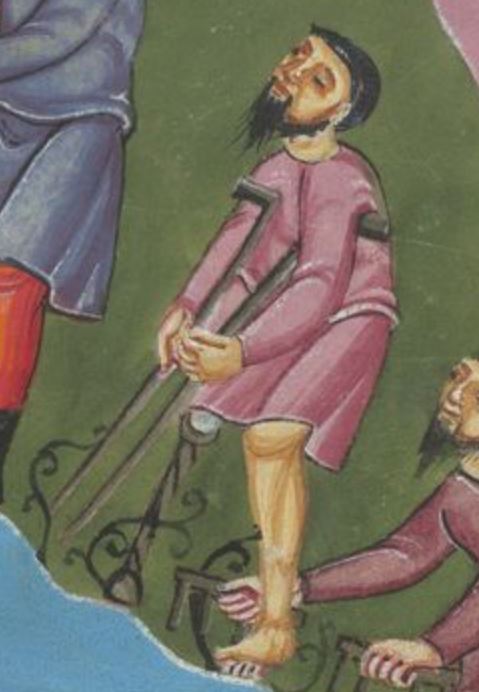
In terms of iconography, the earliest evidence of the use of lower limb prostheses are scenes on Roman vases, the earliest of which dates from the 4th century BC (Binder 2016: 30; Sellegren 1982: 13). Other pictorial documents come from The Psychomachia Codex from St Lawrence (KBR MS. 10066-77) from the 10th century, which depicts two figures with amputated legs. Other scenes date back to the High Middle Ages, when they often appear in illuminations and mosaics of the 12th-14th centuries. In particular, these are scenes from manuscripts such as the Bury Bible (Corpus Christi MS 002, 1v, 1135-1138, England), the St. Elizabeth’s Psalter (Cividale del Friuli, Sign. Ms CXXXVII, 173r, 1201-1207, Italy), Franco-Flemish Antiphonal (Ms. 44/Ludwig VI 5, f. 202, 1260-1270, France or Belgium), Arthurian Romances (Beinecke MS 229, 257v, 1275-1300, France) and Sachsenspiegel (HAB Cod. Guelf. 3.1 Aug. 2°, 20v, 1350-1375, Germany), but also mosaics such as the mosaic from Lescar Cathedral (1120 -1141, France). As far as can be judged from this sample, amputation above the knee practically did not use prostheses and patients move with the help of sticks, while amputations below the knee could be replaced by a simple and uniform leg with an eye at the end. The prostheses appear to be wooden or metal, and the stump is inserted into a hole that is padded on the side facing the ground. The same type of prosthesis (bent-knee prosthesis) was used until relatively recently and is still recommended for children in developing countries, but as a temporary and emergency solution, which causes muscle dystrophy, and therefore it is necessary to exercise the muscle thoroughly after using the prosthesis (Werner 1987: 625). Above prostheses and walking sticks, we can find a number of wooden walkers and attachment platforms in medieval iconography, both without projections and with projections replacing the limb, for those afflicted with leprosy or polio (Hernigou 2014a; 2014b).

A selection of amputated legs and prostheses of the Middle Ages.
From left: The Psychomachia Codex from St Lawrence (KBR MS. 10066-77), mosaic from Lescar Cathedral (1120-1141, France), The Bury Bible (Corpus Christi MS 002, 1v, 1135-1138, England), St. Elizabeth’s Psalter (Cividale del Friuli, Sign. Ms CXXXVII, 173r, 1201-1207, Italy), Franco-Flemish Antiphonal (Ms. 44/Ludwig VI 5, f. 202, 1260–1270, France or Belgium), Arthurian Romances (Beinecke MS 229, 257v, 1275-1300, France), Sachsenspiegel (HAB Cod. Guelf. 3.1 Aug. 2°, 20v, 1350-1375, Germany).
Written materials are also good sources. The most striking evidence of the existence of prostheses is the characteristic bynames, which reflects the appearance of the owner. From the Scandinavian area, we know the byname viðleggr (“wooden leg”) and three men with the byname tréfótr (“wooden leg”) who lived in the 9th-13th centuries. We also know the word spituleggr, which can refer to a wooden or thin leg (Jónsson 1908: 220, 222). Old Norse knows the phrase ganga á tréfótum (“to walk on wooden legs”), which means “to be in a bad condition” (Baetke 2006: 662). We also know bynames related to the use of wooden prostheses from Middle High German as well: stelzære, stelzner, uf dir stelzen, râvôt (Keil 2012: 372).
Probably the best written accounts of early medieval wooden prostheses revolves around a Norwegian named Ǫnundr, who lived at the turn of the 9th and 10th centuries. While Landnámabók (Sturlubók version, ch. 161) only says that Ǫnundr “(…) fought against King Harald in Hafrsfjord and lost his leg. He then sailed to Iceland and took the land (…) “, Grettis saga (ch. 2-11) presents a more colourful account – Ǫnundr is portrayed as a viking who accidentally learns of a sea battle in Hafrsfjord and decides to take part in it. King Harald’s men cut off almost his entire leg below the knee, but Ǫnundr is saved by his comrades, who disengage from the battle and flee. “Ǫnundr recovered, but he walked with a wooden leg all his life. Therefore, as long as he lived, he was called Ǫnundr the Wooden Leg” (Grettis saga 2). After his wound healed, Ǫnundr went to the Hebrides, but he suffers from psychological problems – he is silent, aware of his poor mobility, missing a leg and losing his joy in fighting, which he also reveals to his friend. A friend advises him to settle down and find a wife, but the father, whom they jointly propose to his daughter, is reluctant to marry his daughter to a disabled person with no real estate. However, he is assured that Ǫnundr can move about without difficulty and that he has plenty of chattels and a good lineage, which boosts Ǫnundr’s confidence and sets off on further raids. In the ensuing battle, his friends place a log under his leg so he can engage as well, and his opponent’s weapon gets stuck in the log, which Ǫnundr uses to defeat the opponent. Then Ǫnundr sails to Ireland, where he engages in other war actions, and after a stop in the Hebrides, where he gets married, he then goes to Norway, where he takes revenge on the usurpers of his land. He then goes to Iceland, where he accumulates property and builds a family. At the time of his death, he is considered the bravest and most skilled man with a prosthesis in the collective consciousness – “There never lived a one-legged man in Iceland who was braver and more skilled than him” (Grettis saga 11). Another Icelander with a prosthesis known from Eyrbyggja saga (ch. 18) was Þórir the Wooden Leg – he was said to have been struck in the thigh but survived the injury and walked with a wooden leg for the rest of his life, adding that he had a marriage and offspring. Gísla saga (ch. 2) also mentions Skeggi, who was hit by a spear in the leg and used a wooden prosthesis after losing the limb.
Codex Aureus of Echternach (GNM, Hs. 156142, 77v).
Although these stories may be modified by oral and later literary tradition, the relevant information sounds realistic. While evidence suggests it was common for the disabled to be cared for at home (Grettis saga 4), individuals who were considered fit by society of the time were able to return to living independently and contributing to society to great effect, despite a society that in many ways wrote them off as incomplete. The stakes were high: only through risky ventures could unmarried youths increase their wealth and status, and thus enter the marriage market, start a family, and begin building their own estate (Raffield et al. 2017). On Ǫnundr’s example, we can observe that hits to the lower part of the legs were common. The sources hardly say anything about the prostheses themselves, but we do know that they were made of wood.
Acknowledgment and dedication
The article we have presented here was consulted with the surgeon and reenactor Zbyňek Buchtela, whom we thank for his stimulating comments. Swedish reenactor Erik Hörnsten also deserves thanks for mentioning an interesting find from the Varnhem monastery. We would like to dedicate this article to Michael Kahn, Reece M. Nelson and Vojtěch Šlapák.
We hope you liked reading this article. If you have any question or remark, please contact us or leave a comment below. If you want to learn more and support our work, please, fund our project on Patreon, Buymeacoffee or Paypal.
Bibliography
Landnámabók = Landnamabók I-III: Hauksbók, Sturlubók, Melabók. Ed. Finnur Jónsson, København 1900.
Gísla saga = Sága o Gíslim. Přel. L. Heger. In: Staroislandské ságy, Praha 1965, 133–185.
Grettis saga = Saga o Grettim. Přel. L. Heger, Praha 1957.
Eyrbyggja saga = Sága o lidech z Eyru. Přel. L. Heger. In: Staroislandské ságy, Praha 1965, 35–131.
Magnús saga góða = Sagan af Magnúsi góða. Edited by N. Linder – H. A. Haggson. In: Heimskringla Snorra Sturlusonar III, Uppsala 1872. Available here.
Njáls saga = Sága o Njálovi. Přel. L. Heger. In: Staroislandské ságy, Praha 1965, 321–559.
Baetke, Walter (2006). Wörterbuch zur altnordischen Prosaliteratur, Greifswald. Available here.
Baumgartner, René (1982). Fußprothese aus einem Frühmittelalterlichen Grab aus Bonaduz – Kanton Graubünden/Schweiz. In: Medizinisch orthopädische Technik 102, 131-134.
Bennion, Elisabeth (1980). Antique Medical Instruments, Berkeley – Los Angeles.
Binder, M. – Eitler, J. – Deutschmann, J. – Ladstätter, S. – Glaser, F. – Fiedler, D. (2016). Prosthetics in antiquity – An early medieval wearer of a foot prosthesis (6th century AD) from Hemmaberg/Austria. In: International Journal of Paleopathology 12, 29-40.
Bogin, Barry – Varela-Silva, Maria Inês (2010). Leg Length, Body Proportion, and Health: A Review with a Note on Beauty. In: International Journal of Environmetal Research and Public Health, vol. 7 (3), 1047–1075.
Cueni, Andreas (2009). Die frühmittelalterlichen Menschen von Aesch (Anthropologische Untersuchungen). In: Hartmann, C. – Cueni, A. – Rast-Eicher, A. (eds.). Aesch: ein frühmittelalterliches Gräberfeld, Luzern, 83-126.
Czarnetzki, A. – Uhlig, C. – Wolf, R. (eds) (1983). Menschen des Frühen Mittelalters im Spiegel der Anthropologie und Medizin. Würtembergisches Landesmuseum, Stuttgart.
Claspe, Jon – Ramasamy, Arul (2013). Traumatic amputations. In: British Journal of Pain 7 (2), 67–73.
de Godoy, J. M. P. – Vasconcelos Ribeiro, J. – Andrioli Caracanhas, L. – de Fátima Guerreiro Godoy, M. (2010). Hospital infection after major amputations. In: Annals of Clinical Microbiology and Antimicrobials, 9:15.
Erdem, H. – Tetik, A. – Arun, O. – Besirbellioglu, B. A. – Coskun, O. – Eyigun, C. P. (2011). War and infection in the pre-antibiotic era: the Third Ottoman Army in 1915. In: Scandinavian Journal of Infectious Diseases 43, 690–695.
Finch, Jacky (2018). The complex aspects of experimental archaeology: the design of working models of two ancient Egyptian great toe prostheses. In: Draycott, Jane (ed.). Prostheses in Antiquity, London, 29-48.
Friedmann, L. W. (1972). Amputation and Prostheses in Primitive Cultures. In: Bulletin of Prosthetics Research (BPR) 10-17, 105-138.
Frölich, Annette (2011). Medical Tools from the First Millennium – A New Recognition after Reinterpretation of Artifact Material. In: Boyé, Linda (ed.). Det 61. Internationale Sachsensymposion 2010, Haderslev, Danmark, Neumünster, 317-324.
Gennarelli, T. A. – Champion, H. R. – Sacco, W. J. – Copes, W. S. – Alves, W. M. (1989). Mortality of patients with head injury and extracranial injury treated in trauma centers. In: Journal of Trauma and Acute Care Surgery 29, 1193–1201.
Hernigou, Philippe (2014a). Crutch art painting in the middle age as orthopaedic heritage (Part I: the lepers, the poliomyelitis, the cripples). In: International Orthopaedics 38 (6), 1329–1335.
Hernigou, Philippe (2014b). Crutch art painting in the Middle Ages as orthopaedic heritage (part II: the peg leg, the bent-knee peg and the beggar). In: International Orthopaedics 38 (7), 1535–1542.
Holck, Per (2009). The Skeleton from the Gokstad Ship: New Evaluation of an Old Find. In: Norwegian Archaeological Review, 42:1, 40-49.
Janoušek, Jakub (2015). Četnost a možnosti řešení amputací dolních končetin. Univerzita Karlova v Praze : Fakulta tělesné výchovy a sportu.
Jónsson, Finnur (1908). Tilnavne i den islandske oldlitteratur. In: Aarbøger for Nordisk Oldkyndighed og Historie 1907, Kjøbenhavn, 161–381.
Keil, Gundolf (2012). Heilkunde bei den Germanen. In: Beck, H. – Geuenich, D. – Steuer, H. (eds.). Altertumskunde – Altertumswissenschaft – Kulturwissenschaft: Erträge und Perspektiven nach 40 Jahren Reallexikon der Germanischen Altertumskunde, Berlin – Boston, 317–388.
Klaphake, S. – de Leur, K. – Mulder, P. G. H – Ho, G. H. – de Groot, H. G. – Veen, E. J. – Verhagen, H. J. M – van der Laan, L. (2017). Mortality after major amputation in elderly patients with critical limb ischemia. In: Clinical Interventions in Aging 12, 1985-1992.
Matzke, J. K. W. (2011). Armed and Educated: Determining the Identity of the Medieval Combatant, University of Exeter.
Mays, S. A. (1996). Healed limb amputations in human osteoarchaeology and their causes: a case study from Ipswich, UK. In: International Journal of Osteoarchaeology 6, 101–113.
Meri, J. W. (2005). Medieval Islamic Civilization: An Encyclopedia, New York – London.
Mitchell, P. D. (2004). Evidence for elective surgery in the Frankish states of the near east in the crusader period (12th-13th centuries). In: Jankrift, K. P. – Steger, F. (eds.). Gesundheit–Krankheit: Kulturtransfer Medizinischen Wissens von der Spätantike bis in die Frühe Neuzeit, Cologne, 121-138.
Pavlačková, Markéta (2012). Kvalita života pacientů po amputaci na dolní končetině. Masarykova univerzita : Lékařská fakulta. Bakalářská práce.
Price, Neil S. (2002). The Viking Way: Religion and War in Late Iron Age Scandinavia, Uppsala.
Rau, B. – Bonvin, F. – de Bie, R. (2007). Short-term effect of physiotherapy rehabilitation on functional performance of lower limb amputees. In: Prosthetics and Orthotics International 31 (3), 258 – 270.
Raffield, B. – Price, N. – Collard, M. (2017). Male-biased operational sex ratios and the Viking phenomenon : an evolutionary anthropological perspective on Late Iron Age Scandinavian raiding. In: Evolution and Human Behavior, vol. 38, no.3, 315–324.
Rhyne, C. E. – Templer, D. I. – Brown, L. G. – Peters, N.B. (1995). Dimensions of suicide: perceptions of lethality, time, and agony. In: Suicide & Life-Threatening Behavior 25(3), 373-380.
Runcie, Harriet (2015). Infection in a Pre-Antibiotic Era. In: Journal of Infectious Diseases & Preventive Medicine 3 (2), 125.
Sahu, A. – Sagar, R. – Sarkar, S. – Sagar, S. (2016). Psychological effects of amputation: A review of studies from India. In: Industrial psychiatry journal 25 (1), 4-10.
Sellegren, Kim R. (1982). An Early History of Lower Limb Amputations and Prostheses. In: Iowa Orthopedic Journal 2, 13–27.
Sexton, John P. (2010). Difference and Disability: On the Logic of Naming in the Icelandic Sagas. In: Eyler, Joshua R. (ed.). Disability in the Middle Ages: Reconsiderations and Reverberations, London – Burlington, 149-163.
Smith, P. W. – Watkins, K. – Hewlett, A. (2012). Infection control through the ages. In: American Journal of Infection Control 40, 35-42.
Štefan, I. – Stránská, P. – Vondrová, H. (2016). The archaeology of early medieval violence: the mass grave at Budeč, Czech Republic. In: Antiquity, 90, 759-776.
Thordeman, Bengt (1939). Armour from the Battle of Wisby: 1361. Vol. 1 – Text, Stockholm.
Van Cant, Marit (2018). Surviving Amputations: A Case of a Late-Medieval Femoral Amputation in the Rural Community of Moorsel (Belgium). In: Turner, W. J. – Lee, Ch. (eds). Trauma in Medieval Society, Leiden, 180–214.
van der Mark, Wiel (2016). A Broken Leg in the Year 1350: Treatment and Prognosis. In: EXARC Journal, 2016/2.
Vlasatý, Tomáš (2017). „Ryji runy léčby“ : Runové modlitby a léčitelství starého Severu. In: Projekt Forlǫg : Reenactment a věda.
Available here: https://sagy.vikingove.cz/ryji-runy-lecby/
Werner, David (1987). Disabled Village Children. A Guide for Community Health Workers, Rehabilitation Workers, and Families, Palo Alto.
Westphalen, Petra (2002). Die Eisenfunde von Haithabu, Die Ausgrabungen in Haithabu 10, Neumünster.
Williams, M. W. (1920). Social Scandinavia in the Viking age, New York.
Woosnam-Savage, R. C. – DeVries, Kelly (2015). Battle Trauma in Medieval Warfare: Wounds, Weapons and Armor. In: Tracy, Larissa – DeVries, Kelly (eds). Wounds and Wound Repair in Medieval Culture, Leiden, 27–56.


